By Heather Veeder, MD, Regional Medical Director, VITAS Healthcare
This article was published in January 2022 and updated in April 2024.
Heart failure (HF), which affects over 37 million people worldwide, is a major cause of morbidity and mortality, especially among older adults.
HF is classified by left ventricular ejection fraction (EF); the American College of Cardiology and American Heart Association categorizes HF as such:
- Heart failure with reduced ejection fraction (HFrEF) - EF ≤40%
- Heart failure with borderline ejection fraction (HFbEF) - EF 41%-49%
- Heart failure with preserved ejection fraction (HFpEF) - EF ≥50%
These different subcategories of HF have different clinical characteristics, and while EF is a major differentiator when guiding management and treatment of HF, there does not appear to be major differences in mortality and prognosis between EF subgroups, as shown in a study by Shah, et al. published in the Journal of the American College of Cardiology.
According to the study, heart failure is associated with markedly lower median survival, poor long-term prognosis, and increased risk of cardiovascular and heart failure admission, regardless of ejection fraction classification.
Median Survival of Patients Hospitalized with HF
The study analyzed data from the GWTG-HF (Get With The Guidelines–HF) registry and claims data from the US Centers for Medicare and Medicaid Services (CMS), and thus examined data from 39,982 patients from 254 hospitals admitted for HF between 2005 and 2009.
These patients, who were all fee-for-service Medicare beneficiaries age ≥65 years hospitalized with a diagnosis of HF, were divided by HF subgroup:
- 18,299 (45.8%) had HFpEF
- 3,285 (8.2%) had HFbEF
- 18,398 (46.0%) had HFrEF
The study examined the median survival of patients hospitalized with HF compared to the general population. It also examined 5-year outcomes between different EF groups, including mortality, all-cause readmission, cardiovascular readmission, heart failure readmission, and the composite mortality/readmission rate.
Regardless of EF, median survival for patients with HF was similar and declined with advancing age. Within each age group, median survival for patients with HF was significantly lower the general US population, as seen in the figure below:
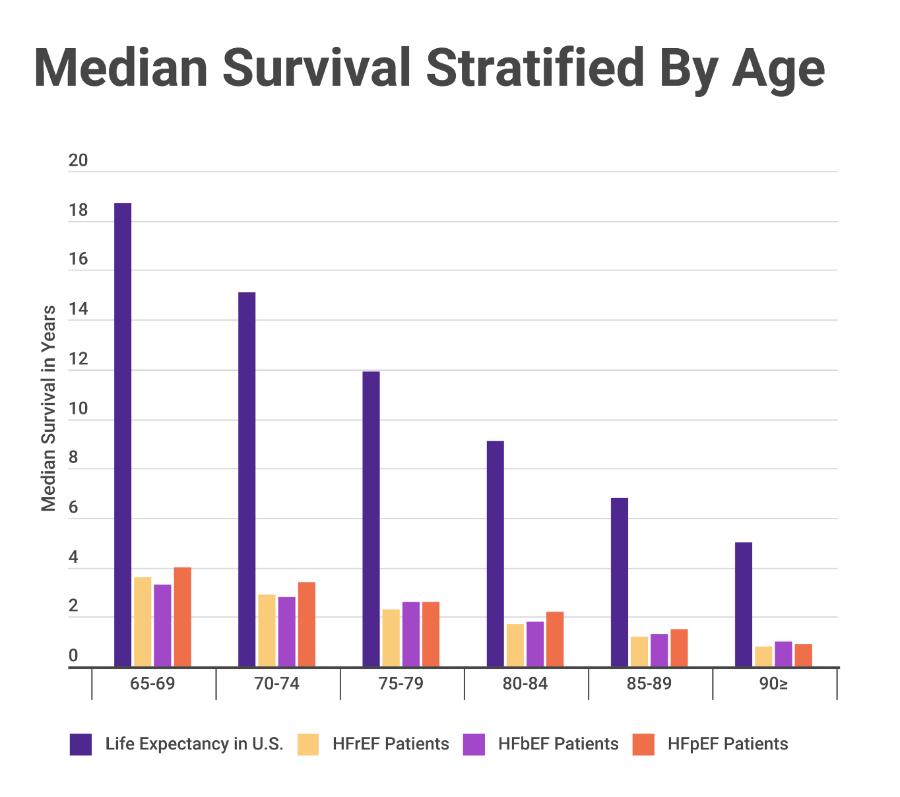
For example, among patients 65 to 69 years of age, median survival was ≤4.0 years. In contrast, according to the National Vital Statistics Report for the general US population, the median survival of individuals 65 to 69 years of age is 18.7 years. In this age group, patients with HF lost up to 15 years of life.
Examination of mortality data across all age groups shows similarly markedly lower median survival rates among patients with HF compared to that of the general individual life expectancy in the United States, with median survival for patients with HF roughly 5 times shorter than the general population.
Mortality, Readmission Rates Were Similar in All Groups
The findings in this study show that in this very large national registry-based HF patient cohort, mortality and readmission rates were similar in all groups irrespective of EF classification with and without risk adjustment. The figure below compares five-year outcomes:
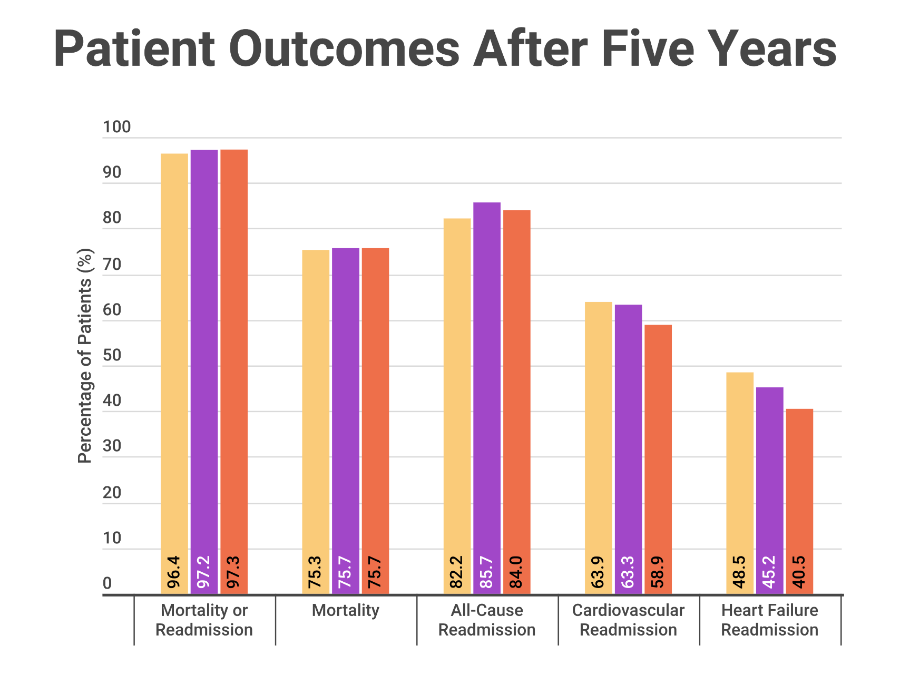
There was no significant interaction between time and EF groups for any of these outcomes. These similarities across EF groups held true even when adjusting for patient demographics, medical history, examination findings, laboratory findings, and medications, as well as when looking at event-free patients who survived the first 6 months or 1 year post-admission.
The authors of this study conclude that "in patients age ≥65 years hospitalized with HF, 5-year risk of all-cause mortality is high regardless of EF, and the median survival is substantially lower than the general population of similar age."
Hospice Addresses Heart Failure's Complex Challenges
Heart failure is a clinical syndrome with significant morbidity and mortality. It places a substantial burden on both patients and health care systems. Patients with HF bear a heavy disease burden, making them prime candidates for hospice.
As the study by Shah, et al. shows, mortality is high and prognosis is poor in HF patients regardless of EF subgroup classification. Rehospitalization rates for all-cause, cardiovascular, and HF readmission are also high between EF subgroups.
While clinicians use EF classification to make decisions regarding management and treatment of HF, EF categorization is not a requirement for hospice admission; a diagnosis of HF is sufficient.
Hospice is uniquely equipped to address the complex challenges that advanced HF presents. There is ample opportunity in the population of hospice-eligible patients with HF, regardless of their EF classification, for hospice to potentially provide reduction in morbidity and disease burden, reduction in hospitalization and readmission rates, and increase in patient and family satisfaction.
Shah, et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. Journal of the American College of Cardiology. 70.20: 2476-2486.


